If i was him. I will stay at the airport until the office open and try to nego to get the fastest flight home. As the other friend get theirs,it is worth trying. But i noe,deep inside his heart,he fed up already to get back home. Maybe his mind and heart is more toward the exam. I was there once. And i noe how it felt. But i still wasting 4 to 5 hours of my precious time wasted at the KK, and sacrifice all the exercise that i used to do just because i might endanger our little one. I still cant believe it
kelIsya

Monday, October 22, 2012
Thursday, October 11, 2012
Rasmi ergo baby carrier
Yeay..tgh ari td posmen dtg anta ergo baby carrier. Hu3. Terkejut posmen tgok harga barang. Bg mommy,yg tbk utk anak mommy stakat yg mommy mampu.
Ptg ni jgk rasmi pg tesco. Bes sgt!!! Freedom felt. Anak mommy tdo jer.harap amru syg jg slesa dlm ni.nnt ad mase kte posing ngn tweet yr.. Biar daddy jeles.. (yeke??)
Tuesday, October 9, 2012
Amru fakhry 50 days
Mommy sayang amru fakhry.. Nt ad masa mommy slow citer psl syg eh. Nt besar2 mommy xingat dah.hehe.. 50 days n sayang dah kateh; bak kata tok we :)

Thursday, August 25, 2011
surgery exam yr 5
Examiner: Mr Ramzi
Wad 7C
For the history, CQ should be in patients own word and use medical terms in HOPI. Eg: patient complained of blood in the urine for 7 years. HOPI hematuria was associated with severe flank pain. Stenting and ESWL was done 10x and 3 operation was perform however the symptoms did not improved.
For examination, as patient is day 1 post op-PCNL, so patient refused to lie down.
Patient had nephrostomy tube at the back on the left side, 10 cm from the spinous process and 15 cm infrascapular. The NT tube drain 1500ml hematuria and cast seen in the tube. Otherwise, no pus no stone in the urinary bag.
My impression is, patient has left renal stone and was treated with PCNL.
DISCUSSION
Q: why you said it is renal stone not ureteric or bladder stone
A: history of flank pain and hematuria, history of ESWL and had neprostomy tube.
Q: what is the risk factor for renal stone?
A:1) high oxalate diet. Eg:chocolate milk, black tea, soy, yogurt
2)dehydration
3) stasis in infection or tumor.
4)urinary ph: urate and oxalate in acidic urine and struvite and phosphate in alkaline urine.
5)endocrine abnormality-eg: hyperPTHàhypercalcemia.
6)metabolite imbalance: hyperuricemia à uric acid stone.
Q: if there is a male presented with flank pain and hematuria, how you will investigate??
A: specific investigation, I would like to perform KUB x-ray which is 90% sensitive for the renal stone
Q: if you cannot see stone on x-ray, what are other modalities:
A: ultrasounds. Ultrasound can pick up uric acid stone and xanthine stone.
IVU
Q: you had treated this patient with PCNL. What advice you can give to the patient to prevent recurrent.
A: 1) I will investigate if for the uric acid level, PTH and calcium level to exclude endocrine and metabolite problem and treat accordingly if present.
2)dietary recommendation- I would advice patient to drink adequate water, drink more citrus juice and avoid high oxalate diet, high protein diet and high dose of vit C
Q: what is the complication if you do not remove the stone.
A:The stone can lead to obstruction àinfection. Obstruction also can lead to hydronephrosis and patient later will developed renal failure.
Q: what will happened of this patient develop renal failure (this question is little bit tricky ^_^)
A: as long as the right kidney is normal, patient would not develop any sign or symptoms.
Q: what is the investigation specifically to look for renal damage. Not blood investigation.
A: renal scan. Scincitograpy.
Ok.. lets moved to the short case J
Q: examine the abdomen
A: abdomen is distended at the lower part below the umbilicus……………on deep palpation there is a mass palpable at the pelvic are. The mass irregular surface, hard in consistency and ill-defined margin. No pulse palpable I cannot go below the mass but can go above it. The mass is fix. On percussion the mass is dull.
Q: how to differentiate between pelvic or abdominal mass?
A: can go above it or below it. As the patient, I cannot go below it, so likely the mass is pelvic origin.
Q: how to percuss pelvic mass
A: from the xiphisternum to the symp pubis.
Q: generally, how the patient look? And what is your diagnosis
A: generally, patient is cachexic and lethargic and the conjunctiva and oral mucosa is pale. I think patient hand pelvic cancer which might be bladder ca, ovarian ca or uterine ca.
SEKIAN.selamat berpuasa and selamat beramal di akhir ramadhan. Semoga bertemu lagi pada ramadhan akan datang and kite semua menjadi insan yang lebih baik and berkhidmat kepada masyarakat. insyaAllah semua orang jadi doctor pada ramadhan akan dtg, last word, kalo ada kekurangan dalam script ni jangan segan2 betulkan atau tambah. Hope all of us will benefit from it.
Sunday, August 14, 2011
duodenal ulcer
kissing ulcer : there is both anterior and posterior duodenal ulcer
anteriorly placed ulcer tend to perforate
posterior duodenal ulcer tend to bleed, by eroding a large vessel such as gastroduodenal artery
anteriorly placed ulcer tend to perforate
posterior duodenal ulcer tend to bleed, by eroding a large vessel such as gastroduodenal artery
Saturday, August 13, 2011
Traube's space notes
Gastroenterology:Traube's space
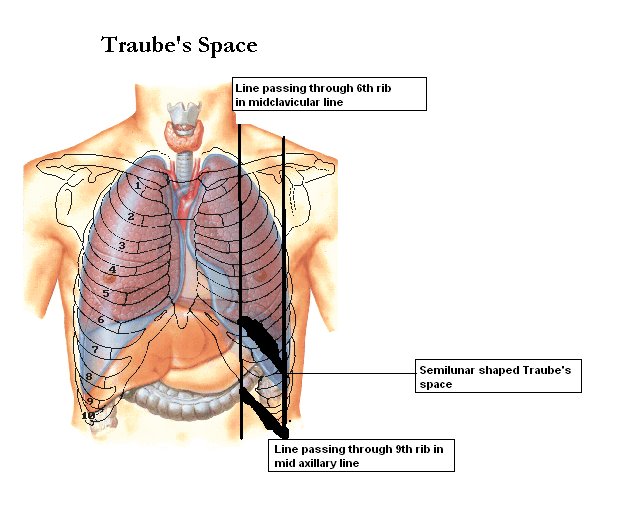
Surface Markings
1. Draw two vertical lines one passing through the 6th rib in the midclavicular line and the next passing through the 9th rib in midaxillary lines.
2. Now draw a smooth curving line with convexity upwards ftom the sixth rib in midclavicular line to 9th rib in midaxillary line.
3.Draw another straight line passing through the costal margin from 6th rib to 9th rib.
All these boundaries enclose a near semilunar space called Traubes space.
Anatomical boundaries are:
1. Right : Lateral margin of left lobe of liver.
2. Left : Spleen.
3. Superior : Resonance of lung.
4. Inferior : Costal margin.
Contents
1. Fundus of stomach (Hence percussion of Traubes area normally gives Tympanitic resonance).
2. Costo-phrenic recess of left pleura devoid of lungs.
Causes of obliteration of Traubes space:
1. Full stomach.
2. Left sided Pleural effusion.
3.Splenomegaly.
4. Enlargment ofleft lobe of liver due to any etiology.
5. Dextrocardia.
6. Proloiferative growth in fundus of stomach.
Note: A left lung mass lesion/consolidation alone never produces impairment as lung is not extending to traube's space.
traubes-space on clinicalmedicineupdate
Monday, July 18, 2011
papilledema
causes of papilledema
edema and hyperemic of the optic disc
- raised ICP
- malignant hypertension
- cavernous sinus thrombosis
Grade I papilledema is characterized by a C-shaped halo with a temporal gap

With Grade II papilledema, the halo becomes circumferential

Grade III papilledema is characterized by loss of major vessels AS THEY LEAVE the disc (arrow)

Grade IV papilledema is characterized by loss of major vessels ON THE DISC.

Grade V papilledema has the criteria of grade IV plus partial or total obscuration of all vessels of the disc.

reference: dorland dic, OHCS, eye rounds.org
Subscribe to:
Posts (Atom)